ReadPaper Blog
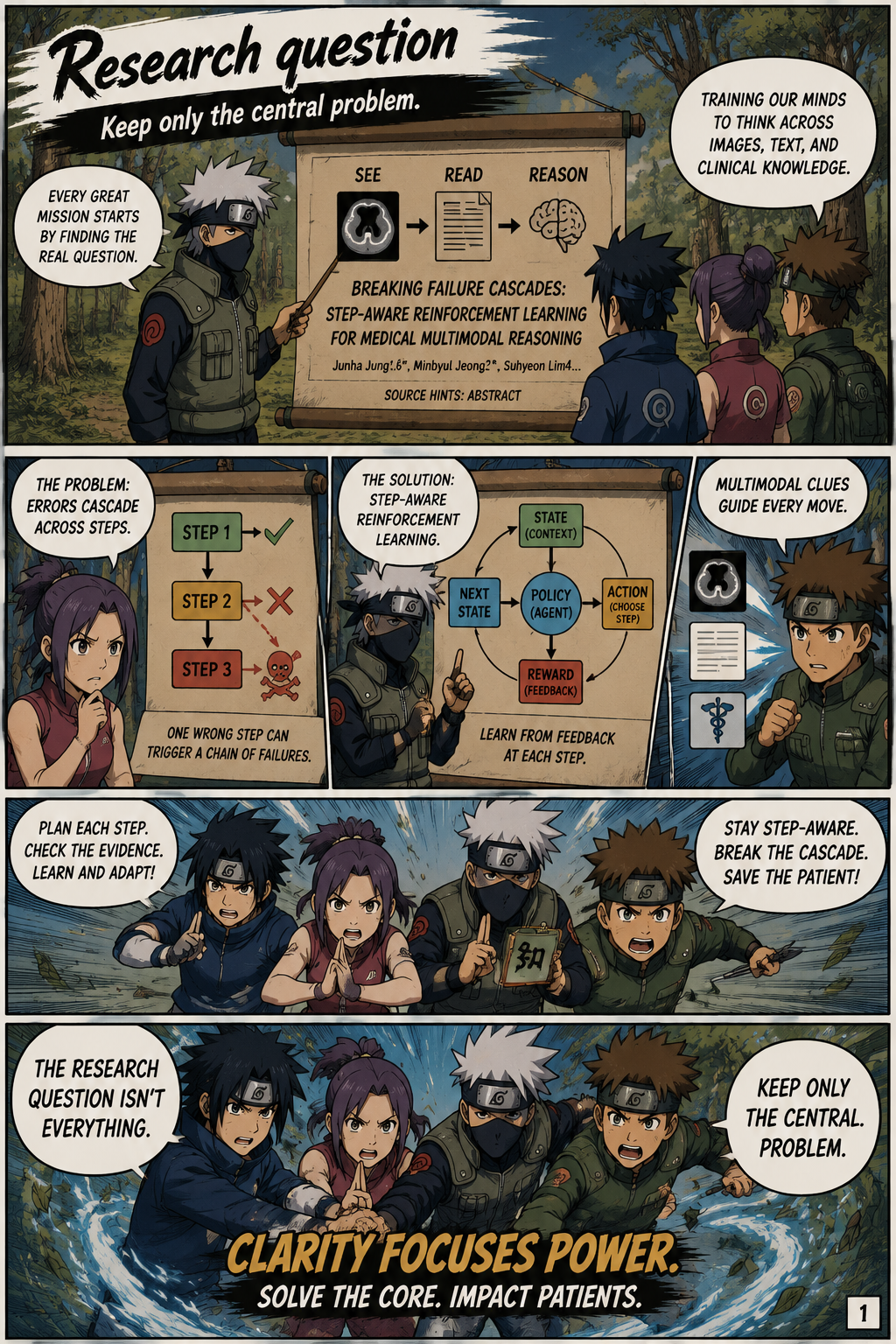
Breaking Failure Cascades: Step-Aware Reinforcement Learning for Medical Multimodal Reasoning
This paper studies why multimodal large language models fail on open-ended medical visual question answering, arguing that early mistakes in clinical reasoning often cascade into wrong final answers. It proposes Medical Reasoning-aware Policy Optimization (MRPO), a reinforcement learning method that uses step-wise process rewards and stronger penalties for earlier invalid reasoning steps, improving both answer accuracy and reasoning quality across medical VQA benchmarks.
Source: (none provided)
Research question
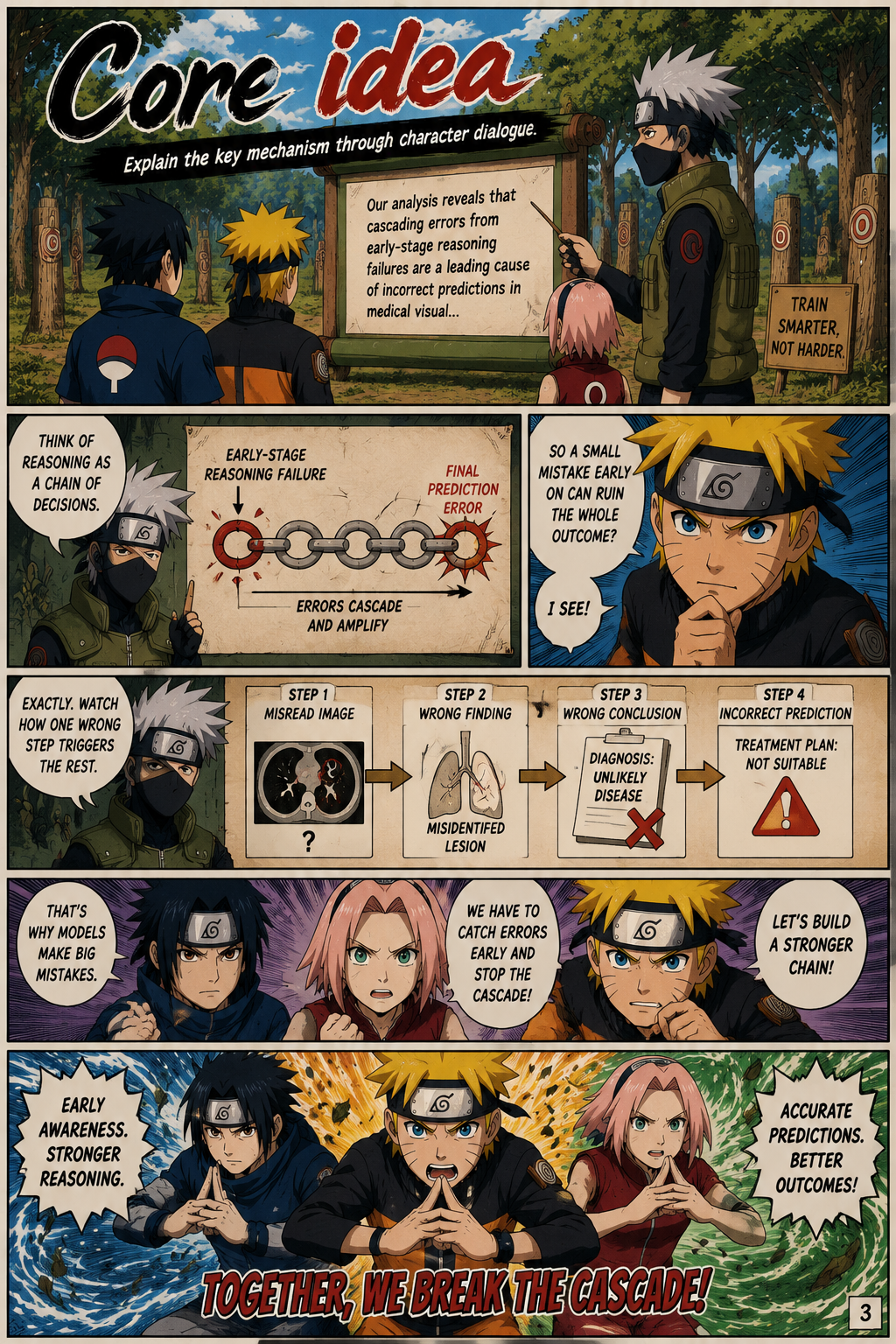
The paper addresses a practical weakness in medical multimodal reasoning: models may generate plausible-looking chains of thought while making an early clinical or visual inference error that derails the final diagnosis or answer. Its central motivation is that clinical image reasoning is not only about choosing the correct final response, but also about maintaining valid intermediate observations about anatomy, pathology, and evidence in the image. The authors focus on open-ended medical visual question answering, where sparse final-answer rewards provide little guidance about which part of a generated reasoning trace went wrong. They identify failure cascades as a structural error pattern in which one invalid reasoning step increases the likelihood of later invalid steps. This framing matters because medical MLLMs need reliable reasoning trajectories, not merely high aggregate accuracy on closed-form benchmarks.
Why old methods fall short
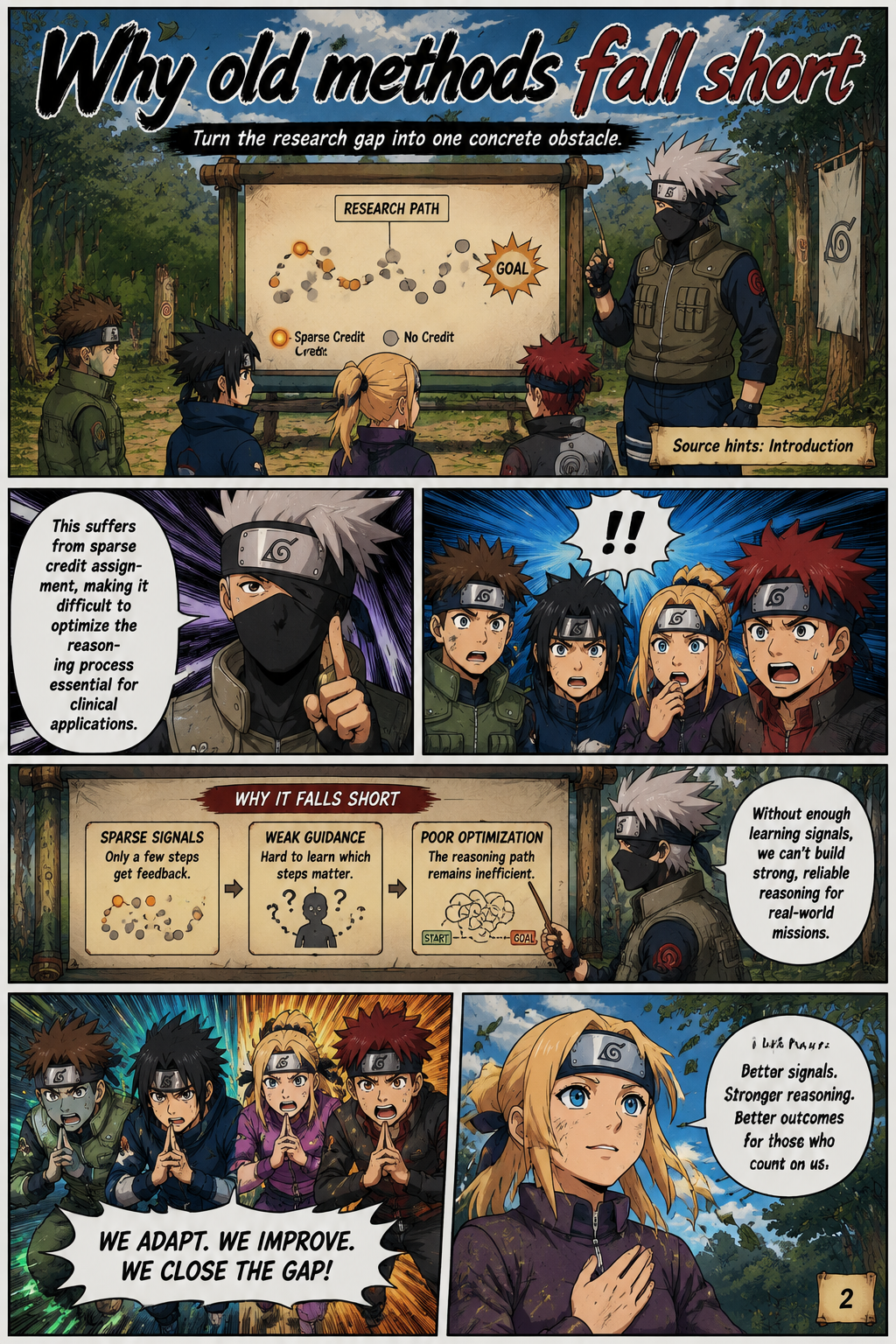
Existing post-training methods for medical multimodal large language models are described as largely outcome-centric, relying on final answer correctness or sequence-level preferences. The paper argues that this creates a sparse credit assignment problem: when a generated response is wrong, the training signal is spread across the whole sequence rather than tied to the specific reasoning step that caused the error. This limitation is especially severe in free-form clinical generation, where rewards are delayed until the entire answer is complete. Prior chain-of-thought fine-tuning and GRPO-style reinforcement learning can improve medical reasoning behavior, but they do not directly identify the location of a failed step in the reasoning trajectory. The authors therefore position step-level supervision as necessary for models that must reason through open-ended clinical images.
Core idea
The paper’s core empirical insight comes from analyzing sentence-level reasoning traces with two measures: First Failure Point (FFP) and Failure Accumulation Rate (FAR). FFP captures where the first invalid reasoning step appears relative to the full trace, while FAR measures how often later steps fail after that first error. Across Qwen3-VL-8B-Instruct, InternVL3-8B-Instruct, HuatuoGPT-Vision-7B, and Lingshu-7B on VQA-RAD, SLAKE, and PathVQA, earlier first failures are associated with substantially higher incorrect-answer rates. The authors evaluate step validity using GPT-5-mini with two complementary criteria, Gold Alignment and Answer Contribution, and report substantial agreement with human judgments in their validation. This evidence supports the claim that wrong answers often emerge from the temporal structure of reasoning failures rather than from isolated final-step mistakes.
Evidence check
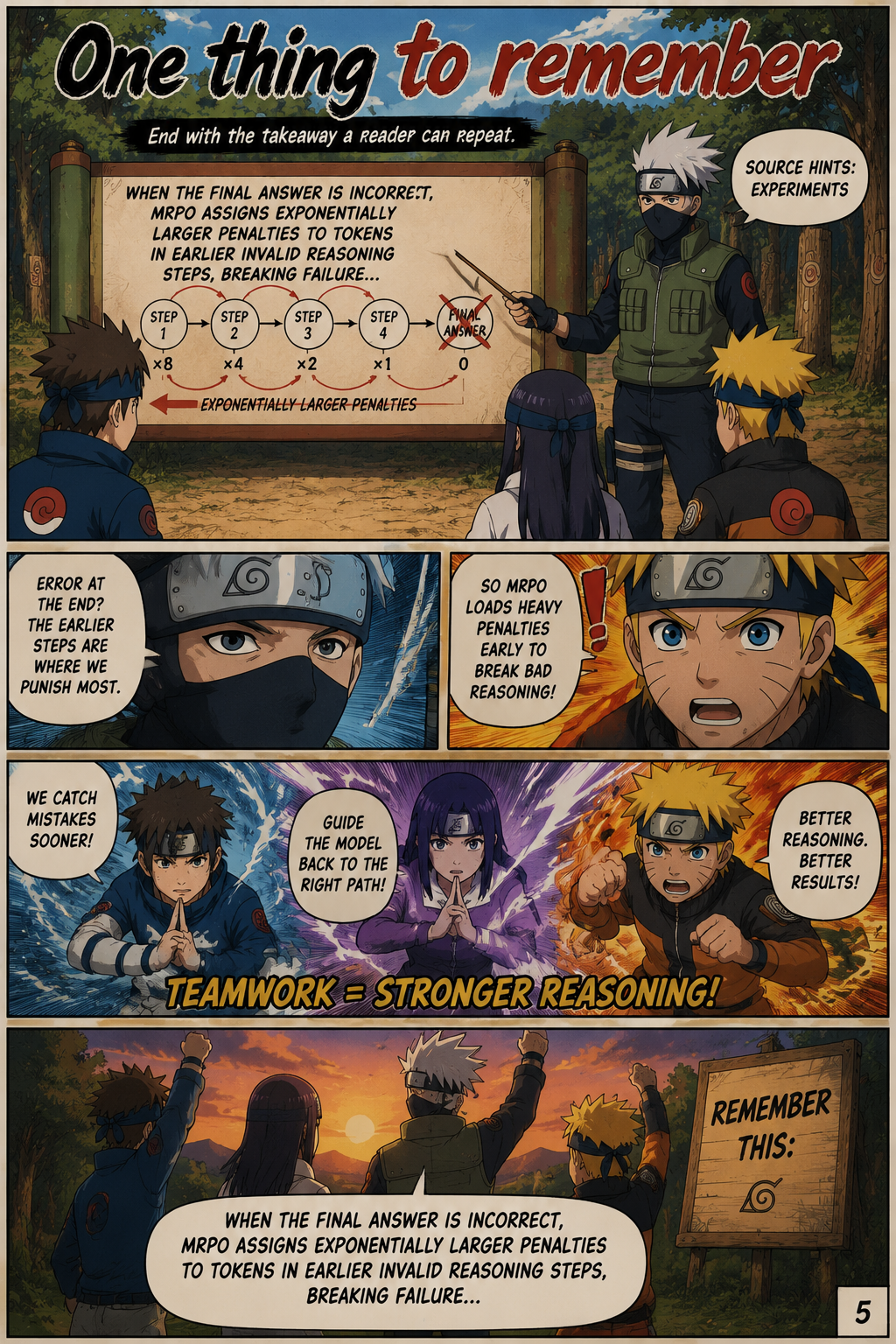
Medical Reasoning-aware Policy Optimization, or MRPO, is introduced as a GRPO-based reinforcement learning algorithm that reshapes the advantage signal using both answer rewards and step-wise reasoning process rewards. An external judge model evaluates each reasoning step as valid or invalid, while the answer reward determines whether the final prediction is correct. When the answer is wrong, MRPO assigns exponentially larger penalties to tokens in earlier invalid reasoning steps, so the learning signal targets the point where the cascade begins. Successful reasoning trajectories are preserved rather than penalized indiscriminately, which distinguishes the method from uniform sequence-level punishment. In effect, MRPO combines medical step-level evaluation with token-level credit assignment to make the model less likely to repeat the first invalid clinical inference.
One thing to remember
The experiments apply MRPO to Qwen2.5-VL-7B-Instruct, Qwen3-VL-8B-Instruct, and InternVL3-8B-Instruct using 13K training samples and evaluate performance on diverse open-ended medical VQA benchmarks. The method consistently outperforms standard GRPO and the recent GDPO reinforcement learning baseline across the tested backbones. On Qwen3-VL-8B-Instruct, MRPO is reported to exceed larger medical MLLMs such as HuatuoGPT-Vision-34B by 2.79 points, suggesting that targeted reasoning supervision can compete with scale-heavy medical instruction tuning. The failure analysis is equally important: MRPO reduces early-stage reasoning failures from 64.0% to 13.0%, indicating that the method changes the model’s reasoning pattern rather than merely tuning final-answer behavior. The main implication is that medical MLLM training should optimize where and why reasoning fails, not only whether the final answer matches a reference.